Introduction
Cerebral vascular malformations (CVMs) are of clinical importance because of their propensity to cause intracerebral hemorrhage (ICH) and/or seizures.1,2 Arteriovenous malformations (AVMs) and cerebral cavernous malformation (CCM) are the most frequent forms of CVMs. Epileptic seizures are a frequent manifestation of both AVM and CCM3 but its importance is often overlooked in favor of ICH, which is the most frequent and feared component of a CVM’s natural history.4 Seizures are however debilitating and adversely impact the quality of life.5 The incidence of seizures as presenting complaint in AVM and CCM is 30% and 47% respectively in hospital-based studies.2
Predisposing factors for seizures in AVM include male gender, younger age, temporal or frontal lobe location, AVM nidus diameter >3 cm, superficial or cortical location, middle cerebral artery feeders, absence of associated aneurysms, presence of a venous varix/varices, and superficial venous drainage.6–9 Similarly, in CCM, supratentorial location, cortical involvement, and, interestingly an archicortical/mesiotemporal localization is more frequently associated with seizures.10–13
The exact pathomechanism inciting seizures in CVM remains uncertain. To explain the pathophysiology of epilepsy in patients with AVM, haemodynamic alterations, hemosiderin deposits and vascular remodeling of malformation have been implicated,9,14 while in CCM, a few studies have evaluated the angioarchitectural features of CVMs and their relationship with epileptic seizures.5,15 However, most studies have focused on the alterations in angioarchitecture, that is, the constituent vessels participating in the malformation, but not much attention has been focused on the changes in the perilesional tissue and adjacent cortex, particularly the neuronal and glial components that could directly contribute to seizure induction.
Insights into the specific histomorphological factors associated with seizures could aid in elucidating pathomechanism of epileptogenesis and play a role in predicting the surgical outcome.16 In this study, we evaluated angioarchitectural factors, alterations in perilesional tissue and neuroglial/stromal elements of the perilesional cortex in AVM and CCM to ascertain its contribution to seizures.
Methods
Patient selection criteria and cohort composition
We reviewed all cases diagnosed as AVM and CCM at the Department of Neuropathology, National Institute of Mental Health & Neurosciences, Bangalore, India over a 2 years period between 2015 and 2016. Institutional review board approval obtained. We included cases of AVM and CCM with and without seizures for comparison, as our primary aim was to decipher the angioarchitectural and histomorphological differences that underlie epileptogenesis.
Inclusion criteria
(1) Cerebral lobar lesions-we restricted to lobar lesions to eliminate selection bias, as the location of the lesion is a known risk factor associated with seizure and (2) cases which were subjected to surgical resection with adequate perilesional tissue and adjacent cortex for evaluation.
Exclusion criteria
(1) Midline, deep gray matter nuclei and brainstem lesions; (2) inadequate tissue for histopathological analysis; and (3) cases with prior surgery or embolization. Clinical, imaging and histological characteristics of patients with AVM and CCM with & without seizures were reviewed.
AVM-imaging assessment
The angioarchitecture of the AVM nidus/CCM was defined by a combination of magnetic resonance imaging (MRI) and digital subtraction angiography (DSA). For each AVM the angioarchitectural characteristics examined included: (1) location; (2) feeding artery-number (single/multiple), presence or absence of hypertrophy of the feeding artery (increase in the diameter of the vessel by more than 50%), feeding artery aneurysm, and steal phenomena; (3) nidus-size of the lesion (small <3 cm; medium 3–6 cm; large >6 cm) based on Spetzler-Martin grading scale,17 presence or absence of bleed, aneurysm/fistula (absence of intervening nidus between the artery and vein); (4) draining vein-number (single/multiple), length of leptomeningeal course of the vein (short <2 cm; medium 2–4 cm; long >4 cm) reference to be given, superficial or deep, presence or absence of aneurysm/stenosis; and (5) adjacent parenchyma-presence/absence of hemosiderin deposits, inflammation, gliosis.
CCM-imaging assessment
(1) Location, size of the lesion (<3 cm, 3–6 cm, and >6 cm), number-single/multiple; (2) type of CCM based on Zabramski classification on MRI;18 and (3) presence or absence of post contrast enhancement, perilesional hypointensity, blooming on gradient/susceptibility weighted imaging (SWI) images and gliosis.
Histopathology
Histological characteristics were evaluated using Hematoxylin and Eosin, masson trichrome stain for collagen, Perls Prussian blue stain for hemosiderin, Verhoff’s van gieson stain for elastic fibres. Indirect immunohistochemsitry was performed using GFAP (1:200, 6F2, Dako, Rockville, MD, USA), Neu N (1:500, A60, Merck Millipore, Temecula, CA, USA), phosphorylated neurofilament (phospho NF-1:200, 2F11, Dako). Angioarchitectural changes in vessels-sclerosis of the vessel, thrombosis, intraluminal calcification. In AVM, proportion of arterial, venous and arterialized veins were assessed. (1) Changes in perilesional tissue-hemosiderin deposits, gliosis, reactive astrocytosis, inflammation, calcification, infarction, fibrosis and side-rotic vessels. Siderotic vessels are perilesional thin walled blood vessels with hemosiderin deposition on the vessel wall; (2) Adjacent cortex-dyslamination and dysmorphic changes in neurons were studied using GFAP, Neu N, and Phospho NF respectively; (3) each parameter Rajeswarie RT, et al. Epileptogenesis in CNS Vascular was assessed as present or absent; and (4) gliosis was subjectively graded as mild, moderate or severe.
Statistical analysis
Statistical analysis was performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA). Categorical variables were compared using chi-square test. p-value of less than 0.05 was considered statistically significant. Univariate logistic regression analysis was performed to identify the radiological and histomorphological features associated with seizure presentation.
Result
During the 2 years study period, 41 were diagnosed as AVM. Seizure was the initial presenting symptom in 16 (39%). There were 15 cases diagnosed as CCM during the same period, of which seven (46.6%) had seizures as the presenting complaint. Of these, 24 AVM and eight CCM had sufficient perilesional cortex to be included in the study.
We examined 24 patients with AVM, 18 male (75%) and six female (25%). The age at the time of diagnosis ranged from 14 years to 62 years (mean, 28.9 years). Initial clinical manifestations were seizure in 12 patients (50%), headache in eight (33.3%), focal neurological deficit in three (12.5%) and one patient was asymptomatic. We also examined eight patients with CCM, seven male and one female. The age at the time of diagnosis ranged from 18 years to 40 years (mean, 27.8 years). Initial clinical manifestations were seizure in five patients (62.5%).
AVM topographic and angioarchitectural features on radiology
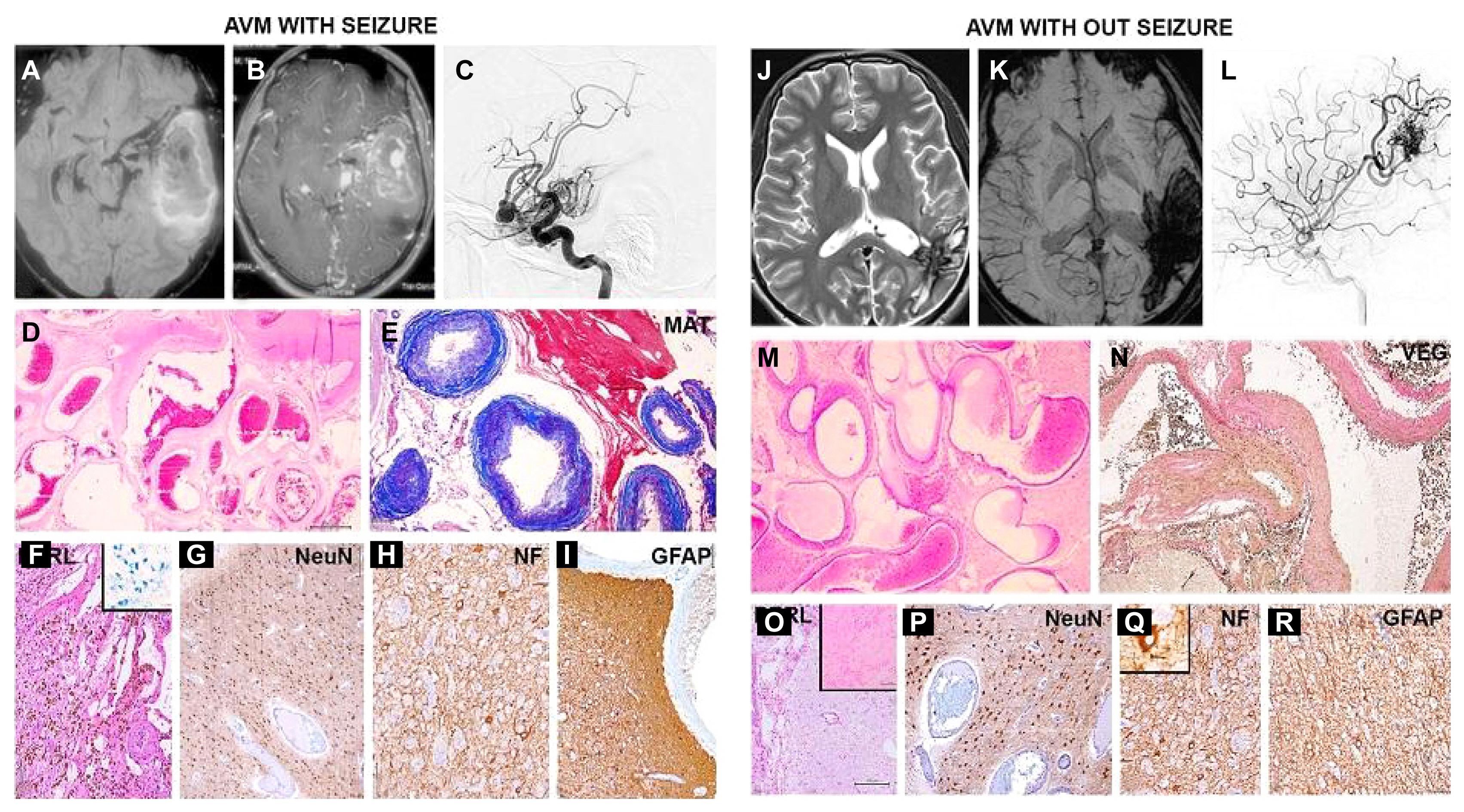
The topographic and angio-architectural features of AVM on radiology are summarized in Table 1. Most patients were in the age range of 21–40 years (62.5%). Males were most commonly affected (75%). Frontal lobe was most common location (33.3%), followed by the temporal lobe (29.2%). No statistically significant difference was noted in demographic characteristics, or location between those with and without seizures. We had selected only those with lobar lesions to remove any confounding factor, as it is well established that superficial lobar lesions are commonly associated with seizure and our primary aim was to decipher the changes in these lesions and the adjacent parenchyma that cause epileptogenesis. The angioarchitectural features of 21 cases of AVM on both MRI and DSA were analyzed by univariate logistic regression, and none of the features were found to be significantly associated by seizure (Fig. 1A–C, J–L).
Histomorphological features of AVM
AVM revealed conglomerate of arteries, arterialised veins and veins in the nidus. The proportion of each component varied with arterial component predominating in 58%, venous in 42%. The vasculature of the vasoformative lesion revealed varying degrees of mural thickening, calcification, acquisition of elastic fibres in arterialized veins (Fig. 1D, E, M, N). The adjoining tissue revealed gliosis, inflammation, calcification, and infarction in event of steal phenomenon. Extent of hemorrhage varied with evidence of fresh and old bleed (Fig. 1F). We analyzed the histomorphological features of the lesion, perilesional tissue and the adjacent cortex in detail and compared findings between patients with and without seizures, summarised in Table 2 and Fig. 1.
We observed that hemosiderin deposition (Fig. 1F) and gliosis (Fig. 1I) of the perilesional tissue was more common in patients presenting with seizures compared to those without seizures (Fig. 1O, R) and the difference was statistically significant (p<0.05). No difference between the groups was found with other lesional/perilesional features like sclerosis of vessel, thrombosis, proportion of the AVM component, bleed, inflammation, fibrosis, infarction, calcification and cortical changes like dyslamination/dysmorphic changes in cortical neurons (Fig. 1G, H, P, Q).
Fig. 1 angioarchitectural features and changes in perilesional tissue of AVM with and without seizures on radiology and histomorphology.
CCM topographic and angioarchitectural features on radiology
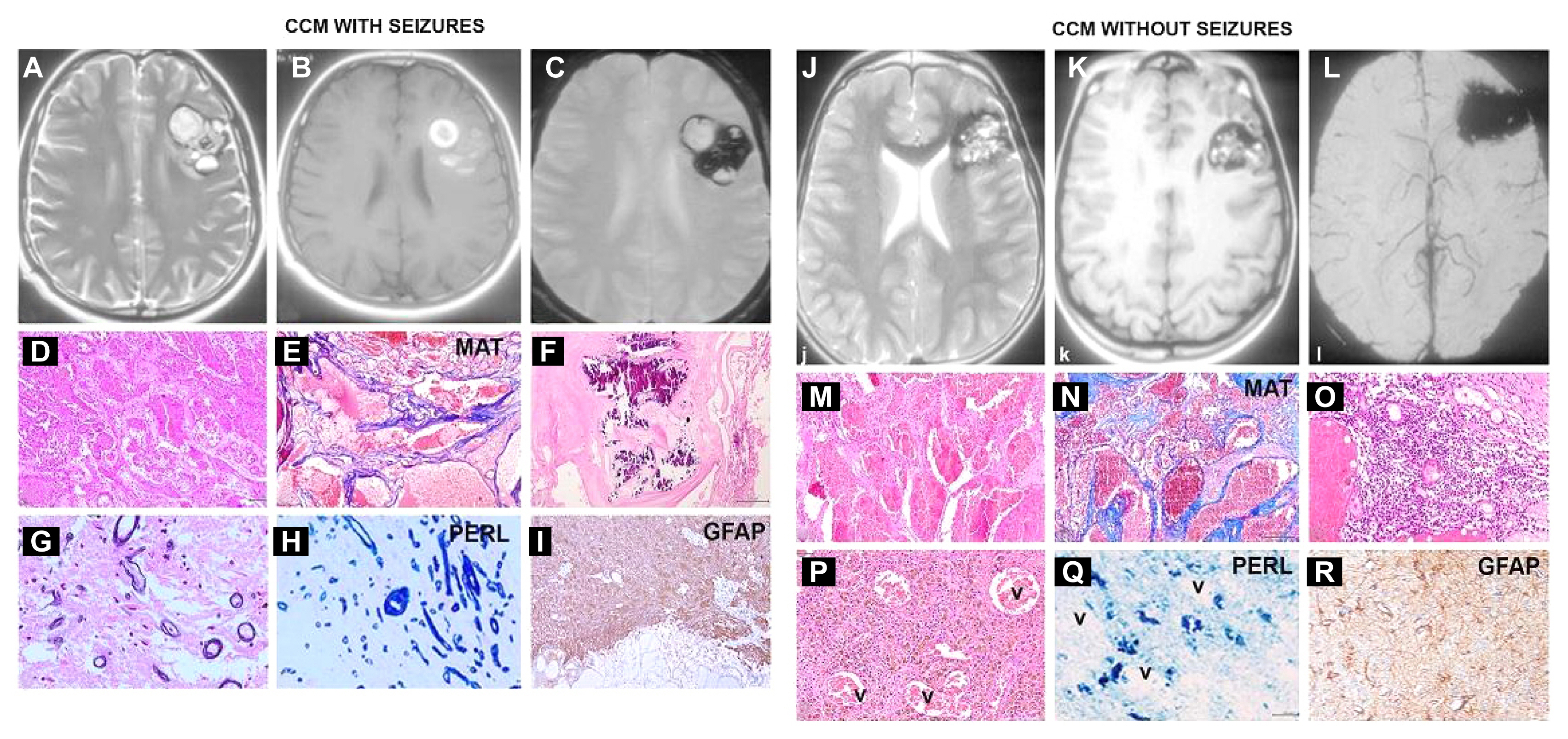
The topographic and angioarchitectural features of CCM based on radiology is summarized in Table 3, Fig. 2 A–C, J–L). The age range was 21–40 years (75%). Males were more commonly affected (87.5%). Frontal lobe was most common site (62.5%), followed by temporal lobe (37.5%). Statistical analysis showed no significant differences between demographic characteristics, or angioarchitectural features between patients with or without seizures.
Histomorphological features of CCM
CCM were characterized by back to back arranged thin venous channels lined by flattened endothelium (Fig. 2D, E, M, N). No parenchymal insinuation was seen between the vessels. The vessels demonstrated varying degree of vascular sclerosis, calcification and intraluminal thrombi/phleboliths (Fig. 2D, N). The lesions were often accompanied by fresh and old hemorrhage with hemosiderin (Fig. 2P) eliciting parenchymal inflammation (Fig. 2O), reactive astrocytosis, gliosis (Fig. 2I, R) and siderotic vessels (Fig. 2G, H), tissue infarction in immediate surrounding parenchyma. The adjacent cortex revealed glial and neuronal changes. Comparison of the findings between the group with and without seizures yielded interesting results, summarized in Table 4.
Interestingly, siderotic vessels in the perilesional tissue was observed exclusively in the cases with seizures (Fig. 2G, H) and absent in those without seizures (0/3 vs. 5/5, p<0.01) (Fig. 2P, Q). Bleed and hemosiderin deposition were common to all cases (Fig. 2P, Q). Perilesional changes like gliosis (Fig. 2I, R), reactive astrocytosis, sclerosis of vessel, inflammation, fibrosis, infarction, calcification (Fig. 2F), and cortical changes like dyslamination/dysmorphic changes in cortical neurons did not show any statistical difference between the two groups.
Fig. 2 angioarchitectural features and changes in perilesional tissue of cerebral CCM with and without seizures on radiology and histomorphology.
Discussion
AVMs are abnormal tangles of dilated vessels (nidus) with arterialized veins and veins of varying thickness and caliber lacking an intervening capillary network, which results in direct shunting of high-pressure arterial system and low pressure venous system.
CCMs are sinusoidal vascular channels devoid of muscular and elastic tissue. They are lined by a single layer of endothelial cells that lack intervening tight junctions.2 Both AVM and CCM present with intracerebral hemorrhage, followed by seizures. Other presentations are non-hemorrhagic including focal neurologic deficits, headache, or maybe asymptomatic and detected on brain imaging performed for other reasons.19 In our study, we analyzed the factors associated with seizure in two of the most common types of CVM-AVM and CCM. Seizure was the presenting complaint in 39% of AVM and 46.6% of CCM compared to 29–36% in other series in published literature.6,7,20 These studies noted higher incidence of seizures in younger age group (21–40 years), compared to focal deficits in those aged 60 years and above, which is similar to our study. In addition, male gender had higher predilection for seizures,6,21 as noted in our study in both AVM and CCM (3:1 and 7:1, respectively).
Previous studies identified cortical, temporal superficial nidus locations, superficial venous drainage, length of leptomeningeal course of draining vein, presence of fistula and venous stenosis as predictors of AVM-associated epilepsy.6,7,9,21,22 Large size of AVM (>3 cm) is an independent predictor of seizure (p<0.0001).6,16 In our study, we included only cortical based cases, most in temporal or frontal location with superficial drainage, with no statistically significant difference in patients with seizures. This could be due to our inclusion criteria of evaluating only lobar lesions. We did not find any correlation between the size of AVM and seizures.
Various factors implicated in epileptogenesis in CVM are haemodynamic changes and the alterations in the adjacent neuroglial parenchyma.23 Brain tissue around the AVM is prone for hypoperfusion, due to arteriovenous shunting called as ‘steal phenomenon’ or due to the loss of autoregulation of cerebral circulation.14 Impaired perinidal cerebrovascular reserve cause hypoperfusion-induced remodeling of the perinidal cortex resulting in chronic ischemia, neoangiogenesis, potentiating neuronal excitatory pathways, favoring an epileptogenic mechanism.16,24–26 In our study, the perilesional tissue had higher frequency of hemosiderin deposition and gliosis in the group with seizures. These findings support the hypothesis that in AVM, vascular remodelling, chronic bleed and micro hemorrhages cause hemosiderin deposition in perilesional tissue triggering gliosis, and epileptogenesis. Astrocytes, either through their interaction with excitatory neurotransmitter release or by reducing the antiepileptogenic adenosine content promote epileptogenesis 27–30 Dyslamination of neurons and dysmorphic neurons are associated with seizures in the background of cortical dysplasias, trauma, ischemia.31
Distortion of neuronal lamination and dysmorphic neurons in adjacent cortex were seen in AVM, but occurred with equal frequency in both groups.
Intriguingly, in CCM, these same factors did not play a significant role in seizure causation as hemosiderin deposition was seen in all cases of CCM, with and without seizures. On imaging, they showed heterogenous signal intensity with peripheral hemosiderin rim blooming on gradient/SWI images. There was no statistical difference in their appearance between the groups with and without seizures. The thin walled veins tend to be leaky with a propensity to bleed. However, the presence of siderotic vessels in the adjacent cortex was seen only in those cases presenting with seizures. This is a novel finding in the present study. It is tempting to speculate that the iron/calcium deposits in the vessels might be transported from the endothelial cells into the astrocytic foot processes lining these vessels, and the injured astrocyte may in turn disrupt synaptic function, triggering seizure activity.
Recurrent hemorrhage due to leaky endothelial junctions in CCM causing persistent hemosiderin deposition, contributing to chronic cortical irritation and remodeling of the underlying cerebral cortex and gliosis have been implicated in other studies.32,33 However, none of the previous studies have highlighted the presence of siderotic vessels. In CCM, the hemosiderin deposition induces alteration in the physiologic environment surrounding CCM by abrogating glutamate uptake, causing high-amplitude, complex spontaneous synaptic events. This promotes neuronal hypersynchronization and propagating perilesional excitatory stimuli to other cortical regions.34 The leaky endothelial junctions produce elevated concentrations of serine and glycine in the peripheral zones of CCM35 and perilesional albumin leakage that promote hyperexcitability.36
These findings that perilesional tissue with hemosiderin deposits, and gliosis maybe primarily responsible for seizure causation, suggests extended surgical resection to include the perilesional tissue may achieve a more favorable seizure outcome following surgery.16 The finding by Baranoski et al.37 that surgical resection of AVM led to better seizure control and higher rates of seizure-freedom compared to embolization or radiosurgery,38 may be attributable to the removal of perilesional epileptogenic focus, validating our findings in this study.3,39
We conclude that in CMVs, changes in adjacent cortex promote epileptogenisis rather than the malformation per se, specifically reactive gliosis and hemosiderin deposits in AVM and siderotic vessels in CCM. Our study is the first to report this association of siderotic vessels in CCM with seizures. Insights into specific histomorphological feature associated with seizures provides understanding of the role of vascular and stromal factors. Individualized treatment strategies can then be made based on the clinical presentation and angioarchitectural characteristics and perilesional tissue of the CVM. Extended lesionectomy, including the adjacent gliotic epileptogenic cortex can be recommended for optimal surgical outcome and seizure control. These findings need validation in large cohorts.