Cardiac Abnormalities in Refractory Status Epilepticus-an Exploratory Study
Article information
Abstract
Background and Purpose
Cardiac abnormalities have been reported during ongoing seizures and refractory status epilepticus (RSE). Reduced heart rate variability (HRV) and cardiac arrhythmias may contribute to sudden unexpected death in epilepsy. We sought to explore the utility of electrocardiographic and echocardiographic changes in patients with RSE prognosis and functional outcome.
Methods
Patients of RSE underwent electrocardiogram (ECG), holter, troponin-I (Trop I), N-terminal prohormone of brain natriuretic peptide (NT-proBNP), and 2-dimensional echocardiogram (2D Echo) along with continuous electroencephalogram in first 24 hours and admission. Heart rate changes/arrhythmias, corrected QT interval (QTc) and HRV, ventricular dysfunction or regional motion wall abnormality were studied on 2D Echo. These parameters were also at baseline, at discharge or death and 30 days post discharge.
Results
This prospective observational study conducted over 18 months enrolled 20 patients with RSE, fulfilling the inclusion criteria. Mean age was 47.75±17.2 years with male: female ratio of 1:1. Mean time to presentation from seizure onset was 8.80±7.024 hours. Central nervous system infection (35.0%), autoimmune encephalitis (20.0%) and cerebrovascular disease (20.0%) were the common etiologies. Amongst cardiac injury markers, cardiac enzymes and QTc prolongation were the commonest abnormalities in RSE. Both reduced HRV and presence of cardiac injury markers had significant correlation with poor outcome along with poor Glasgow coma scale (GCS) and modified Rankin scale (mRS) at presentation, and presence of non convulsive status epilepticus (NCSE).
Conclusions
Presence of poor GCS, poor mRS, markers of cardiac injury, reduced HRV and occurrence of NCSE have a consistent correlation with mortality and poor clinical outcome. Therefore, routine assessment of cardiac abnormalities using affordable, easily accessible and non-invasive tools such as ECG, 2D Echo, holter NT-proBNP and Trop I is recommended in RSE patients.
Introduction
As per the International League against Epilepsy task force on classification of status epilepticus, refractory status epilepticus (RSE) is defined as status epilepticus (SE) persisting despite sufficient dose of benzodiazepines and at least one antiseizure medication (ASM), irrespective of time.1 This may continue to super refractory SE (SRSE) when SE continues for 24 hours or more after use of anesthetic therapy, including SE recurring on weaning of anesthesia.1 RSE occurs in 23.0–43.0% and SRSE in approximately 22.0% of patients with SE.2,3 The predominant cause of RSE in developing countries is presumed encephalitis, which is more common in children.2 Central nervous system (CNS) vascular causes, on the other hand, are more frequent in adults and elderly, while metabolic etiology predominates in the elderly. However, in developed countries, the commonest etiology of RSE is stroke followed by drug withdrawal.3,4 The treatment of RSE and SRSE, comprising of ASM like benzodiazepines, sodium valproate, phenytoin, levetiracetam, and others, along with anesthetic drugs such as midazolam, phenobarbital, and propofol that may produce hypotension and respiratory suppression in the intensive care units (ICUs), is challenging.4
SE is a known independent risk factor for mortality. Cardiac complications may additionally contribute to worse outcomes along with increased mortality risk.5 Markers of cardiac injury, cardiac arrhythmias, ventricular dysfunction, and regional wall motion abnormalities (RWMA) have been witnessed in RSE.5 Postictal arrhythmias are also markers of increased sudden unexpected death in epilepsy risk.6 Over the last few decades, many seminal animal studies have been done to study association of cardiac injury in SE and RSE. However, animal data is difficult to translate to human studies. Therefore, this study was planned to diagnose early cardiac injury in patients of RSE with special focus on non-invasive diagnostic modalities and explore their role in prognosis.
Methods
This was a prospective observational cohort study carried out between January 2021 and June 2022 in patients of RSE admitted under Neurology services at a tertiary care institute in Rajasthan in Western India, after clearance by Institutional Ethics Committee (ethical clearance certificate number AIIMS/IEC/2021/3401). Patients were recruited during acute RSE after informed written consent. The inclusion and exclusion criteria were as below. Inclusion criteria: 1) patients with age of 18 or more with or without comorbidities; 2) patients fulfilling diagnostic criteria of RSE;1 and 3) patients willing to provide written informed consent. Exclusion criteria: 1) patients with coronary artery disease or ischemic heart disease; 2) patients with heart failure/cardiomyopathy; 3) patients with congenital heart disease; and 4) patients with prior history of pacemaker/implantable cardiac defibrillator placement.
All patients were assessed for demographic information and clinical details. Laboratory evaluation constituted magnetic resonance imaging brain, cerebrospinal analysis and additional biochemical studies undertaken as dictated by the clinical and radiological features. They were monitored with continuous bedside electroencephalogram (EEG) to assess for electrographic cessation of SE. Additionally, cardiac parameters evaluated were N-terminal prohormone of brain natriuretic peptide (NT-proBNP), troponin I (Trop I), 6 hourly electrocardiogram (ECG), 24-hour Holter and 2 dimensional echocardiogram (2D Echo). Follow-up of above cardiac studies was undertaken at discharge and ECG, 2D Echo done at 30 days post discharge.
Tools
Clinical history
Demographic details of patients including age, gender, education and occupational status were recorded. Details of clinical history and examination included cause and duration of SE, type of RSE, duration of seizure, seizure frequency, number and type of ASM taken, whether known epilepsy or de-novo seizures, prior history of SE, Glasgow coma scale (GCS) and modified Rankin scale (mRS).
Continuous bedside EEG
All patients were admitted in ICU and continuous EEG recording was done using 10–20 international system of electrode placement. EEGs were assessed based on background rhythm, pattern of discharges, burst suppression and presence of electrographic seizures. Non convulsive status epilepticus (NCSE) was defined as changes in behavior and/or cognition from baseline and diagnosed according to Salzburg criteria into definite, probable and possible NCSE.7 Electrographic seizure was defined as a rhythmic discharge or spike and wave pattern with definite evolution in frequency, location, or morphology lasting at least 10 seconds; evolution in amplitude alone did not qualify.8,9 Burst suppression was used to describe an EEG pattern consisting of a continuous alternation between high-voltage slow and/or sharp waves and attenuated (or suppressed) electrographic activity.7–9 The duration of burst, suppression and inter burst interval was noted.
Cardiac monitoring
ECG monitoring: ECG was done immediately on presentation and every 6 hours in first 24 hours of admission for RSE. Arrhythmias such as atrial fibrillation (AF), atrial flutter (AFL), ventricular fibrillation (VF), ventricular flutter (VFL), sinus arrhythmia, sinus pause and asystole were included. Sinus pause was defined as a clearly visible delayed sinus beat, where the following beat is exactly in line with the original rhythm and there is no other visible irregularity in heart rhythm. An asystole was defined as a period without heart beat or ‘p ’ wave lasting at least 3 seconds. Conduction abnormalities included atrioventricular (AV)-block and bundle branch block (QRS-complex widening of more than 0.12s). Repolarization abnormalities comprised of T wave inversion and ST-elevation or depression (equivalent to >2 mm). Bradycardia was defined as heart rate less than 60 beat per minute, tachycardia as heart rate more than 100 beat per minute, significant tachycardia as more than 150 beats per minute and corrected QT interval (QTc) prolongation as QTc more than 450 msec in males and more than 460 msec in females.
Cardiac enzymes: quantitative analysis of cardiac enzymes was done in all patients in whole blood sample. Trop I more than 0.5 mg/mL and NT-proBNP more than 150 pg/mL was taken as abnormal.
Holter monitoring: a 24-hour Holter monitoring study was done in all patients. The changes noted were for sinus tachycardia, sinus bradycardia, AF, AFL, VFL, VF, QTc, ventricular/supraventricular ectopics and heart rate variability (HRV). For HRV, standard deviation of inter-beat interval of normal sinus beats (SDNN) and root mean square of successive differences between normal heartbeats (RMSSD) were studied in 24-hour domain as per European Society of Cardiology and North American Society of Pacing and Electrophysiology.10 SDNN is the mean of standard deviations (SDs) for all R-R intervals, and RMSSD is the root mean square differences of successive R-R intervals. Normative value for SDNN (mean±SD) was 141±39 ms and for RMSSD was 27±12 ms.11 SDNN less than 100 ms was considered abnormal.
2D Echo: bedside 2D Echo was done for all patients by the cardiologist. The parameters assessed were RWMA, valvular defects, atrial and/or ventricular dilatation, left ventricular (LV) and/or right ventricular (RV) dysfunction.
Cardiac injury
Patients were divided into two groups: 1) group with cardiac injury associated with transient LV/RV systolic/diastolic dysfunction, T-wave inversion, ST elevation or ST depression, QTc prolongation, and/or elevated Trop I or NT-proBNP levels and 2) group without cardiac injury. Arrhythmias were not considered directly representative of cardiac injury.
Outcome
Outcomes were determined by mRS and GCS at hospital discharge and 30 days after discharge. Poor functional outcome was defined as mRS score of 4 or higher at discharge and follow up.
Statistical methods
Data was entered in Microsoft Excel sheet and analysed using SPSS 27.0.1 (IBM, Chicago, IN, USA) a value of p<0.05 was considered significant for all statistical tests. Descriptive statistics and univariate analysis were performed. Non-random association between categorical variables such as demographic, clinical and electrographic parameters, cardiac injury, cardiac arrhythmias and reduced HRV, with mortality at discharge and at 30 days follow up, was assessed by Fisher exact test. Significant variables were analysed using multivariate logistic regression analysis and odds ratio (OR) was calculated.
Results
The study included 20 patients with equal distribution of either gender. Mean age of presentation was 47.75±17.2 (range, 22–80) years and median age was 46 years (range, 22–80). Only 55.0% of patients presented within first 24 hours of disease onset, irrespective of seizure type (Table 1). Mean time to admission after onset of disease was 40.50±25.7 hours. However, 17 patients (85.0%) presented to emergency room (ER) within first 12 hours after onset of seizure/SE. Of these, 50.0% presented within 6 hours and seven patients (35.0%) could manage to reach ER within 6–12 hours. The mean time to admission after seizure onset was 8.80±7.0 hours and median was 6.50 hours (range, 1–48). One patient had gone into RSE after 6 hours of admission.
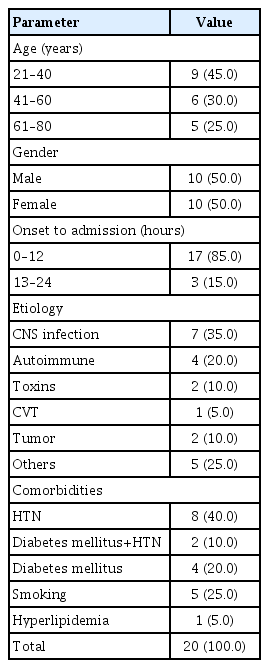
Distribution of patient characteristics in the study
At presentation, 13 patients (65.0%) had poor GCS (less than 8) and 20.0% had GCS of 3. Seven patients (35.0%) had good GCS of 9–15 at presentation. At admission, 17 patients (85.0%) had mRS 5, two patients (10.0%) had mRS 4, one patient (5.0%) had mRS 1 and none had mRS 2 or 3 at presentation. Motor convulsive seizures were initially noted in 18 patients (90.0%) and two patients (10.0%) had non motor seizures (Table 2). Of the 16 convulsive SE (CSE) in ER, 13 converted into NCSE within initial 24 hours. Therefore, 17 patients finally had NCSE within 24 hours after admission and three (15.0%) emerged as SRSE.
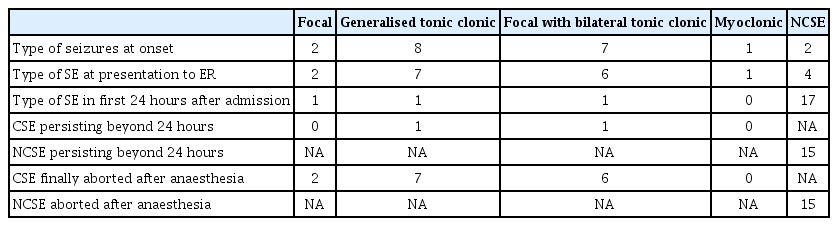
Type of SE and seizure at onset
New onset SE was noted in 80% while four patients had prior history of seizures. All four patients had generalized seizures, three with focal onset and 75% were on ASMs. The causes of RSE were CNS infection (35.0%), autoimmune (20.0%), cerebral venous thrombosis (10.0%), alcohol intoxication, organophosphate poisoning, trauma, hypoxemic brain injury, ischemic stroke and dural arteriovenous fistula (each 5.0%).
The treatment of SE included lorazepam, levetiracetam, valproate, phenytoin, and/or lacosamide. Midazolam infusion was administered in 13 (65.0%), propofol in three, and ketamine in two patients along with ketogenic diet. Although all patients lacked overt/known cardiac disease, 14 (70.0%) had cardiovascular risk factors, and out of these 14 patients with cardiovascular risk factors eight (40.0%) had hypertension, 4 (20.0%) were diabetics and two (10.0%) were found to have both diabetes and hypertension.
Cardiac parameters
The cardiac injury group included 18 patients (90.0%). Cardiac arrhythmias occurred during the course of RSE in nine patients (45.0%) and included sinus bradycardia (n=4, 20.0%), AF (n=2, 10.0%), V tach/VF (n=2, 10.0%), and AV block (n=1, 5.0%). QTc was prolonged in 70.0% (14 patients). Sinus bradycardia occurred in seven patients (35.0%), while all patients were found to have sinus tachycardia. However, significant tachycardia (more than 150 per minute) was observed only in three patients (15.0%). SDNN was normal in two patients (10.0%). SDNN of 50–100 msec (considered ‘at risk’) was found in 10 (50.0%), while less than 50 msec (abnormal) observed in eight patients (40.0%). RMSSD was normal in 11 patients (55.0%) with value 27±12 msec. Amongst 45.0% with abnormal values, 35.0% had RMSSD less than 15 msec and 10.0% more than 39 msec. 2D Echo revealed normal LV and RV function in 16 patients (80.0%); generalized LV and RV dysfunction, which resolved on subsequent studies in two (10.0%); generalized LV dysfunction with subsequent resolution in one (5.0%); and one (5.0%) with inferior RWMA with persistence on subsequent study.
In group A, the most common abnormalities were in the cardiac enzymes. Trop I was raised in 13 patients (65.0%) and NT-proBNP in 12 (60.0%). QTc prolongation was seen in 14 patients (70.0%) followed by generalized LV and RV dysfunction in two (10.0%). Generalized LV dysfunction and ST changes were seen in one (5.0%) patient each. A comparison between groups showed absence of arrythmias in the non-cardiac injury group, while SDNN (p=0.06) and RMSSD (p=0.056) had trend towards significance in those with cardiac injury. All patients were admitted to ICU for management and mechanical ventilation. Anesthetic agents were required in 13 patients (90.0%) for mean duration of 11.09±17.9 days. Mean length of hospital stay was 30.7±22.07 days and median 27 days (range, 2–70). In-hospital mortality occurred in 10 cases (50.0%). Cardiac parameters were compared between those with persistent NCSE beyond 24 hours and those with no NCSE or NCSE less than 24 hours. It was observed that sinus bradycardia, V tach and AV block were significantly more common in those with persistent NCSE beyond 24 hours (Table 3).

Comparison of various cardiac parameters between those with and without NCSE beyond 24 hours
Change of functional outcome
At hospital discharge, functional outcome was poor (mRS 4–5) in nine patients (45.0%) out of 20, excluding in-hospital deaths. However, improvement occurred over time in the subsequent 30 days. Functional outcome improved in five patients, remained same in three, while two patients declined and eventually died. Therefore, final total mortality in RSE at 1-month follow-up was 60.0%. Of the five patients who improved, three changed from poor to good functional outcome (mRS score of less than 3). In terms of GCS, one patient had GCS 3 at discharge, which persisted at 30 days follow up. Three patients (15.0%) had GCS 4–8 and six had GCS 9–15 at discharge. At 30 days follow up, one patient had GCS of 4–8 and seven had GCS 9–15.
Non-cardiac contributors to mortality
There was no association of comorbidities with mortality. Mortality was statistically significantly higher in RSE patients with GCS ≤8 (69.23% [p=0.047] and 79.6% [p=0.032], at discharge and at 30 days follow up, respectively) as compared with good GCS of >8 at presentation. Similarly, mortality in RSE patients with mRS >3 ([52.63% [p=0.007] and 63.15% [p=0.007]], at discharge and at 30 days follow up, respectively) was significantly higher compared with good mRS ≤3 at presentation. When EEG showed persistence of NCSE despite cessation of clinical SE, mortality was 52.94% at discharge and 64.70 % at 30 days follow up (p=0.001 and p=0.005, respectively). Therefore, on univariate analysis amongst non-cardiac parameters, poor GCS, poor mRS at presentation and NCSE were found to have significant correlation with mortality at both time points.
Cardiac contributors to mortality
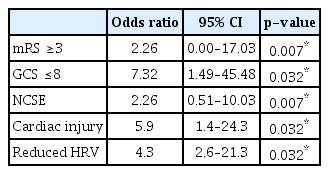
This study did not demonstrate any significant influence of markers of cardiac injury, cardiac arrhythmias or reduced HRV on mortality at discharge. However, cardiac injury markers and HRV were poor prognostic markers of mortality at 30 days post discharge on univariate analysis (Table 4).

Association of mortality at 30 days with various cardiac abnormalities
Final predictors of outcome of RSE by logistic regression
All factors that emerged significant on univariate analysis, were further analysed using multivariate logistic regression. These factors were found to be significant predictors of mortality. Out of all statistically significant parameters, poor GCS followed by presence of NCSE and poor mRS were found to significantly predict mortality at discharge (Table 5). Furthermore, along with poor GCS, poor mRS at presentation, presence of NCSE, presence of cardiac injury and reduced HRV were significant predictors of mortality at 30 days post discharge (Table 6).

Final predictors of mortality in RSE at discharge
Final predictors of mortality in RSE at 30 days
Discussion
The predictors of outcome in RSE have been widely studied across the world. However, there is limited literature on the interplay of RSE and cardiac changes. This observational study focused on evaluating cardiac abnormalities in RSE and their relation to functional outcome. Presence of non-invasive markers of cardiac injury was specifically evaluated along with other factors in RSE.
Demographics and clinical profile of RSE
The demographics of the subjects was akin to regional observations. There was an equal gender distribution similar to regional studies.12,13 This was in contrast to male predominance (male:female, 2.25:1) shown by Dubey et al.14 The third to fifth decade was the predominant age group for RSE in our study. In previous studies, age at presentation ranged from 21–97 years.2,12–15 Ferlisi et al.,16 studying 776 patients from around the world, showed mean age of presentation as 39.8±25.9 years (range, 0–92). On comparison of region-wise data, patients from Asia were significantly younger than those from Europe and the Americas, with mean age of 22.4, 48.2, and 40.5 years, respectively (p<0.001). This relatively younger age of presentation in Asian population was also reflected in our and other Indian studies.14,15
A disconcerting observation was the longer mean time interval from seizure onset to ER presentation (8.80±7.024 hours) than in available literature from developed countries. Mayer et al.4 reported mean interval of 1.3±0.9 hours. On the contrary, studies from the Indian subcontinent reported time intervals of 3.5±2.0 hours and 0.17–160 hours, respectively.12,14 Though we have not looked into specific factors causing this delay, the possible reasons may have been multifactorial. The wide catchment area of the institute located in the desert state of India with low population density and increased travel time from villages would have contributed significantly to the delay. Additionally, scarcity of hospitals in rural areas, lack of specialists in peripheral hospitals and delayed recognition of symptoms both by relatives and health personnel along with local customs and beliefs may have also contributed to the delay.
The greater severity of deficit at admission is suggested by majority (95.0%), having poor presenting mRS of 4–5. In comparison, Hocker et al.17 observed mRS of 5 in four patients (6.5%), mRS 4 in eight (12.9%), mRS 3 in 15 (24.2%), mRS 2 in 10 (16.1%), mRS 1 in 11 (17.7%) and mRS 0 in 14 (22.6%). This implies that majority patients in our cohort came in SE with prolonged generalized seizures and persistence of unconsciousness. Similarly, 65.0% patients had poor GCS. Considering the level of consciousness as predictor of treatment responsiveness at SE onset, Giovannini et al.18 found that 42.0% of treatment refractory RSE had stuporous/comatose presentation (GCS ≤7) compared to only 10.0% who were treatment responsive (p-value <0.005). The same was observed in our cohort with a greater fraction having poor GCS, suggesting a direct correlation with evolution of SE to RSE.
Interestingly, 85.0% had or progressed to NCSE within 24 hours. In most studies of SE, the commonest subtype reported has been generalized SE.4,13,19 Delaj et al.13 observed generalized SE most frequently (41.05%), while NCSE was observed in 7.1% of RSE. Similarly, generalized CSE was found in 73.0% and NCSE in 23.0% by Mayer et al.,4 while Rossetti et al.19 observed generalized CSE in 46.87% and NCSE in 5.2%. On the contrary in an Italian study, 63.0% had NCSE and 10.8% generalized CSE.18 Regional differences have also been observed as Asian patients present with CSE more frequently than NCSE compared to counterparts from Europe and the Americas (71.0%, 53.0%, and 44.0%, p<0.001).16
Cardiac injury in RSE
Our study demonstrated markers of cardiac injury in 90.0% with RSE, which is relatively higher than another similard study (62.9%).5 The most common abnormality in this group was raised cardiac enzymes, either one or both being positive in 90.0%. On the contrary, troponin levels drawn at SE onset were elevated in only 39.1% as noted by Hocker et al.5 Similarly, frequency of patients with raised NT NT-proBNP in RSE was higher in our study than noted by Faria et al.20 (23.0%). QTc prolongation was the next most common cardiac injury marker (70.0%), higher than noted by Hocker et al.5 (22.9%). It was also observed that QTc was increased in patients with ventricular arrhythmias (520.3±87.3 msec) compared with those without (455.9±74.1 msec). Compared to RSE, partial seizures in refractory epilepsy patients were not associated with QTc interval changes.21 Another observation was the rarity of ST changes (only 5.0%) compared with previous studies showing high frequency of ST elevation, ST depression and T wave inversion.6,21,22
On the other hand, cardiac arrhythmias occurred in 45.0% during the course of RSE. Although all patients had sinus tachycardia, significant tachycardia (>150 beats per minute) was present in only 15.0%. In addition, sinus bradycardia (20.0%), AF (10.0%), V tach/VF (10.0%), and AV block (5.0%) were noted. In comparison, Hocker et al.5 reported a higher rate of cardiac arrhythmias in SE (91.4%)-sinus tachycardia (65.7%), sinus bradycardia (48.6%), AF/AFL (20.0%), V tach/VF (11.4%), and AV block (5.1%) with 40.0% requiring intervention. On the contrary, Dubey et al.14 found cardiac arrhythmias in only 2.9%. In another study, cardiac arrhythmias occurred in 35.0% and required intervention in 66.67%, the need for which is correlated with poor functional outcome (p=0.01).18 Most studies thus far have included sinus tachycardia leading to a high prevalence of arrhythmias.5,21,22 However, this dropped to a third when heart rate of more than 150 beats/minutes was considered similar to our observations.22
Interestingly, there is no available literature on effect of HRV in SE and RSE. Thus, the present study is probably the only observation of HRV using SDNN and RMSSD in RSE, with a significant fraction (90.0%) having abnormality in SDNN and 45% in RMSSD.
Predictors of mortality
Our study did not demonstrate any association of demographic variables, cardiovascular comorbidities, or etiological factors with mortality. On the other hand previous studies had shown that age above 60 years, presumed encephalitis or metabolic cause were predictors of poor outcome.14,15,19 On the other hand, mortality was statistically significantly linked with clinical status in RSE, being higher in those presenting with poor GCS ≤8 and poor mRS >3 (69.23% and 53.63%, respectively at discharge as well as 79.6% and 63.15%, respectively at 30 days followup). This was akin to Giovannini et al.18 observation of in-hospital mortality of 42.0% in RSE presenting with GCS ≤7. Hocker et al.17 also reported 31.9% RSE presented with mRS ≥4 at admission with in-hospital mortality of 31.75%.
EEG descriptors such as suppressed background and burst suppression had higher mortality, though not statistically significant. On the contrary, EEG burst suppression was associated with poor functional outcome by Dubey et al.14 and Hocker et al.17 (p=0.01). Likewise, presence of NCSE was a statistically significant predictor of mortality both at discharge and follow up (p=0.001 and p=0.005, respectively). This is in line with similar results where mortality was as high as 86.0% in patients with NCSE.19
Our study also demonstrated a statistically significant association of cardiac injury with mortality at 30 days follow up, though not in-hospital. In a similar study on RSE, mortality in cardiac injury group comprised 45.5%, while it was only 15.4% in those without (p=0.14).5 Likewise, Ibrahim et al.23 showed that mortality rate was higher among patients of CSE with cardiac injury (13.9% vs. 2.6% without) confirming the role of cardiovascular complications in death in CSE.23 In fact, Kurukumbi et al.24 reported that all deaths due to CSE had ECG abnormalities.
In addition, the present study is the only study showing that mortality was higher in RSE patients with reduced HRV with significant correlation with mortality at 30 days.
Final predictors of mortality
The study demonstrated that poor GCS, poor mRS and persistence of NCSE were predictors of mortality at discharge in addition to cardiac injury markers and reduced HRV at 30 days post discharge. This was unlike previous observations of highlighting non-cardiac variables alone as predictors of in hospital mortality. Vooturi et al.25 found fever as the only predictor of death with OR of 8.55. Prolonged duration of ICU stay and prolonged ventilator requirement was also significantly related to poor outcome.12 Similarly, unfavourable Status Epilepticus Severity Score (OR, 2.2) and duration of SE before treatment (OR, 3.35) were poor predictors of RSE.14
The primary limitation of this study is the small sample size of RSE, which was a result of a shorter duration and single center study. Since the institute is a tertiary care hospital, patients admitted were more serious and also had delay in attending our hospital leading to selection bias. The effect of anaesthetic agents on cardiovascular system maybe confounders, though data was acquired in the initial 24 hours of RSE when drug effects were limited. Bradycardia as side effect of sodium channel blockers class like phenytoin and lacosamide was not excluded.
In conclusion, the present study has highlighted that markers of cardiac injury are frequent in RSE. Among these markers abnormalities of cardiac enzymes followed by QTc prolongation were found to be the most common ones. In addition to poor clinical status and persistence of NCSE, abnormal cardiac injury markers and reduced HRV are important poor prognostic markers with high odds for mortality in RSE. Thus, routine analysis of ECG, 2D Echo, holter and cardiac enzymes like NT-proBNP, Trop I as affordable and easily accessible non-invasive tools to observe cardiac abnormalities in RSE patients is recommended. As studies on RSE are not easy, a large sample size with varied presentation, preferably multicenter study, is required for more comprehensive assessment of nature and pathophysiology of cardiac changes in RSE. Future research should prospectively follow up for these patients for longer periods to assess the further evolution of long-term cardiac changes in RSE.
Notes
None.