Epilepsy Surgery in Pediatric Intractable Epilepsy with Destructive Encephalopathy
Article information
Abstract
Background and Purpose:
The aim of the current study is to review the clinical features, surgery outcomes and parental satisfaction of children with destructive encephalopathy who underwent epilepsy surgery due to medically intractable seizures.
Methods:
48 patients who underwent epilepsy surgery from October 2003 to August 2011 at Severance Children’s Hospital have been reviewed. The survey was conducted for functional outcomes and parental satisfaction at least 1 year after the surgery.
Results:
Epileptic encephalopathy including Lennox-Gastaut syndrome and infantile spasms was more prevalent than symptomatic focal epilepsy. Hypoxic ischemic injury accounted for most of the underlying etiology of the destructive encephalpathy, followed by central nervous system infection and head trauma. 27 patients (56.3%) underwent resective surgery and 21 patients (43.7%) underwent palliative surgery. 16 patients (33.3%) achieved seizure free and 27 parents (87.5%) reported satisfaction with the outcome of their children’s epilepsy surgery. In addition, 14 parents (77.8 %) whose children were not seizure free reported satisfaction with their children’s improvement in cognitive and behavior issues.
Conclusions:
Epilepsy surgery in destructive encephalopathy was effective for controlling seizures. Parents reported satisfaction not only with the surgical outcomes, but also with improvement of cognitive and behavior issues.
Introduction
Intractable epilepsy can lead the children who are affected to a catastrophic course, because the seizures are so difficult to control and they are strongly linked to mental retardation.1,2 The major goal of epilepsy surgery in children with intractable epilepsy should be to control seizures, prevent the downhill course of the epileptic encephalopathy (EE), and promote developmental capacities. Therefore, epilepsy surgery should be an early treatment option for the pediatric epilepsy patients with medically refractory seizures, especially in regards to prevention of irreversible cognitive decline and disabilities.3–5
As many other etiological classifications such as malformation of cortical development (MCD), hippocampal sclerosis (HS), tumors and malformation of vascular development, destructive brain lesions including traumatic brain injury, stroke and infections can cause intractable epilepsy. Some of the patients with brain insults suffer not only from intractable seizures, but they also may suffer from the additional global cerebral dysfunction beyond what might be expected from the underlying brain injury alone. Therefore, children with intractable epilepsy caused by destructive encephalopathy can be surgical candidates based on the removal or disconnection of destructive lesions which suspected to be “epileptogenic” after brain insult.6,7
The aim of the current study was to evaluate the clinical features and the seizure outcome in pediatric intractable epilepsy surgery cases of destructive encephalopathy, which were not frequently discussed etiological candidates of epilepsy surgery in children previously. Furthermore, the important changes of the functional outcome and parental satisfaction were considered and assessed in pediatric epilepsy surgery cases.8–11
Methods
48 patients who underwent epilepsy surgery for the treatment of intractable epilepsy with destructive brain lesions at the Severance Children’s Hospital in Seoul, Korea, from October 2003 to August 2011 were indentified. We included the patients whose preoperative magnetic resonance imaging (MRI) findings were compatible with destructive lesions, and we followed up our patients at least 1 year after surgery. One mortality due to immediate postoperative complication was excluded.
48 patients’ information were analyzed; the medical records for demographic data, insult history, presurgical findings, postoperative electroencephalogram (EEG) results and the seizure outcomes. Seizure outcomes were classified according to Engel class; Engel class I-absence of seizures or presence of auras only, or presence of seizures only during drug withdrawal; class II-rare disabling seizures or nocturnal seizures only; class III-worthwhile improvement; and class IV-no improvement.
Intellecutal function was measured using an age-appropriated Wechsler test (K-WISC, K-WAIS) and was presented by verbal IQ (VIQ), performance IQ (PIQ) and full-scale IQ (FSIQ) tests. Infants and severely delayed patients were assessed by the social maturation scale (SMS) composed of the social age (SA) and social quotient (SQ) using Bayley scales.
The functional outcome of the 31 patients and their parental satisfactions by telephone interview, at least 1 year after the surgery, was obtained. The functional outcome in cognition/behavior, motor skills of the patient and parental satisfaction to surgery were scored and classified into five groups: Much improved/very satisfied, improved/satiesfied, no change/with reservation, worsened/unsatisfied and much worse/regret. The postoperative outcome in aspects of the seizure outcome, functional outcome and overall satisfaction of parents were also analyzed .
Statistical analyses were performed with SPSS 18.0 software and group differences in demographic and presurgical factors were tested using independent sample t test, paried t test, Pearson chi-square and Fisher exact tests at the 0.05 level.
Results
Clinical features
Clinical features and demographics were shown in Table 1. Median age at epilepsy was 2.1 years and the age at surgery was 9.1 years. Epilepsy duration to surgery was 5.1 years and median time of follow-up for the patients was 2.7 years. Lead time from the insult to onset of epilepsy was 0.8 years. 45 (93.8%) patients had suffered from daily frequent seizures. Due to the intractability of seizures, 21 (43.8%) of them had a ketogenic diet and 5 (10.4%) patients had steroid treatment at our institution. In terms of clinical spectrum of epilepsy, 33 patients (68.7%) were classified as Lennox-Gastaut syndrome (LGS), 13 patients (27.1%) were in symptomatic focel epilepsy (SFE), and 2 patients (4.1%) were classified with infantile spasms. In terms of etiologic subclassification, the most common etiologies were 32 patients (66.7%) of hypoxic ischemic encephalopathy (HIE), further divided by 17 patients with diffuse hypoxic ischemic encephalopathy (HIE), 7 patients with periventricular leukomalacia (PVL), 8 patients with infarction, followed by 12 (25.0%) with central nervous system (CNS) infection, which was composed of 3 meningitis, and 4 (8.3%) with head trauma.

Characteristics of patients
According to results of magnetic resonance imaging (MRI) lesions, half of the patients had bilateral abnormalities and other half patients had lesions confined to one hemisphere, further divided by 22 multifocal lesions and 2 focal lesions.
Surgical procedures
As shown in Table 2, 27 patients (56.3%) underwent resective surgery; 15 patients of functional hemispherectomy, 9 patients of multilobar resection, 2 patients of cortisectomy, and 1 of unilobar resection. 21 patients (43.8%) underwent palliative surgery, corpus callosotomy. Re-operations were performed in 4 patients (8.3%).
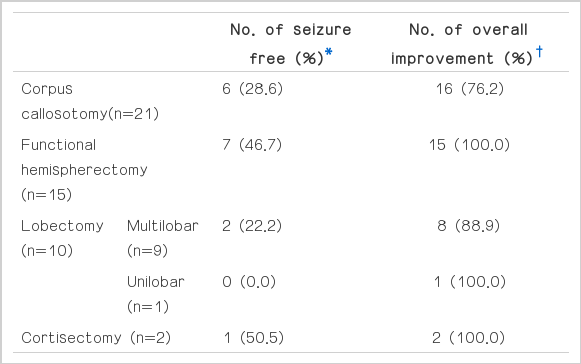
Seizure outcome according to surgical procedures
Seizure outcome
16 patients (33.3%) were categorized as Engel class I, 9 patients (18.8%) were Engel class II, 10 were Engel class III (20.8), and 13 were Engel class IV (27.1%). 42 patients had also categorized as ‘overall improvement’, which was from Engel Class I to IVa.
Among 35 patients classified as epileptic encephalopathy (EE) such as Lennox-Gastaut syndrome (LGS) and infantile spasms, 13 patients (37.1%) achieved an Engel class I outcome. Resective surgery showed relatively higher proportion of Engel class I outcomes compared to palliative surgery procedures. Even considering the overall improvement group, there was a significant difference (26 patients (96.3%) of resective surgery,16 (76.2%) palliative surgery, p= 0.038). There was no significant difference in seizure outcome according to etiology (p=0.818).
Intellectual outcome
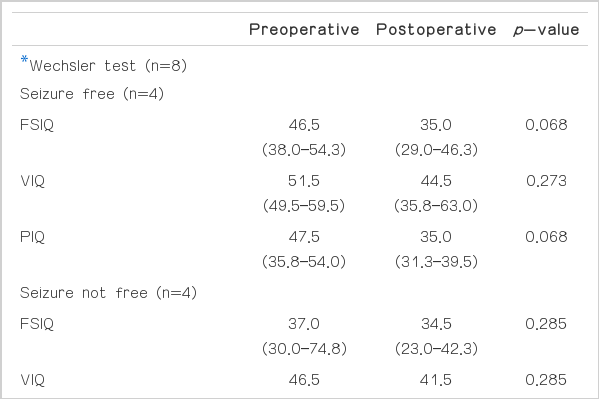
As shown in Table 3, before the onset of epilepsy, 22 patients (45.8%) already had mental retardation caused by brain insults and all the patients had mental retardation before surgery. 20 patients (41.6%) were available to compare both pre- and post-operative cognitive functionality. 8 patients were assessed by Wechsler test, 4 patients from Engel class I had 46.5 full-scale IQ (FSIQ) and 4 patients from Engel class II–IV had 37.0 FSIQ. Among 12 patients assessed by SMS, 6 patients from Engel class I had postoperative 50.3 Social quotient (SQ), and 6 patients from Engel class II–IV had 34.0. Regarding changes between pre- and post-operative cognitive function, the improvement of Social age (SA) in Engel class I patients (N=6) was statistically significant(p=0.028), but other parameters such as FSIQ and SQ in each group were not significantly changed.
Neuropsychological test
Telephone interview showed that 27 parents out of 31 (87.1%) represented overall satisfaction to surgery. All parents of the seizure free group were satisfied with the surgery, and among the remaining 18 parents of seizure present children, 14 (77.8%) were satisfied with the surgery due to improvement in alertness, hyperactivity, concentration, facial expression and responsiveness. And in view of surgical procedures, the satisfaction rate was 83.3% in resective surgery and 92.3% in palliative surgery.
Discussion
Engel class I’s (15 patients, 31.2%) outcome of the current study was a somewhat lower percentage compared to recently reported other surgical series,12–15 but to date, there hasn’t been any one study to analyze epilepsy surgery outcomes focusing on destructive brain lesions. Most of the lesions were bilateral or multifocal MRI abnormalities (46 patients, 95.8%) and a high rate of patients had palliative surgeries (21 patients, 43.8%). However, 42 patients (87.5%) achieved a substantial reduction in seizure frequency and intensity presented as Engel I to IVa. Also, among 35 patients who had EE, 28 patients (80.0%) had achieved resolution of interictal electroencephalogram (EEG) abnormalities such as hypsarrthymia, generalized slow spike and waves (GSSW), and generlaized paroxysmal fast activities (GPFA), which was one of the causes for the mental deterioration of childhood onset EE. Based on these observations, it could infer that even patients who could not achieve an Engel class I outcome could lower their epileptic burden by either lowered seizure frequency and intensity or improvement of interictal EEG abnormalities.16–18
Epilepsy surgery is not indicated for patients with severe diffuse bilateral cortical damage caused by HIE, but there is an increasing interest and number of children who benefit from epilepsy surgery from post HIE damage such as porencephaliccysts and watershed lesions.19
The extent of the brain lesions were different in each patient from focal lesions, multifocal lesions limited in one hemisphere, or bilateral lesions such as periventricular leukomalacia (PVL). Functional hemispherectomy or mutilobar resections were often conducted to multifocal lesions in one hemisphere, palliative procedures for bilateral lesions such as PVL, although curative surgeries were commonly conducted for other structural focal epilepsy. According to the extended location of the lesion, the most appropriate surgical procedure was carefully chosen for each patient.
Destructive brain lesions in pediatrics can be presented by intractable epilepsy. 35 of the patients presented with LGS or infantile spasms, the well known childhood onset epileptic encephalopathy. All had mental retardation as presented by a low IQ score (lower than 70) or DQ (developmental quotient) score (lower than 100) before surgery. This is, as mentiond by Freitag and Tuxhorn,7 the high rate of early onset of epilepsy (=onset within the first and second year of life, 32 patients, 66.7%) and longer duration of the epilepsy (mean 5.1 years) could be the reason for mental retardation in the current study. However, less than half (22 patients, 45.8%) had become mentally retarded due to the destructive lesion itself, and all of them had multifocal and bilateral diffused brain lesions. In other words, 26 patients had additionally become retarded after the onset of severe epilepsy. Therefore, if presented as intractable epilepsy caused by destructive brain lesions, more consideration could be needed for patients who additionally had epileptic burdens caused after the brain insult. In conclusion, it is important to have the proper treatment including epilepsy surgery available to them.
In the current study, quantitative changes in cognition or development after the surgery assessed by formal neurophsychological tests (IQ or SQ) showed no significant differences in even Engel class I outcome patients like other studies.18,20,21 However, as several studies supported, the current study showed improvements in social functioning and behavioral outcomes by their parents’ reports.14,15 In addition, as we could affirm with the phone surgery as shown in Table 4, 87.5% of parents reported satisfaction with the outcome of their children’s epilepsy surgery in regards to cognition, social function and behavior by our structured telephone survey. Even the 77.8% of parents whose children were not seizure free were also satisfied with the epilepsy surgery, influenced by their children’s improvement in alertness, hyperactivity, concentration, facial expression, decreased demand for special care needs and decrease in falling injuries.

Postoperative survey
Limitations of the current study were a small sample size and an inability to telephone survey for all patients. Another limitation was that we had not used the measurements such as the Quality of Life of Children with Epilepsy (QOLCE)13 and the Health-Related Quality of Life in Children with Epilepsy (HRQOLC)14 which could be suitable for evaluating epilepsy-related domains of quality of life, but the current study used our form of survery based on the experience of our institute for telephone survey.
Acknowledgments
The authors have no financial conflicts of interest. We have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.